

Wednesday was World Contraception Day, so I thought it appropriate to bring up type 1 diabetes and contraception. I want to start off by saying that this is an important conversation type 1 diabetics of childbearing age should be having with their doctors, and doctors should be willing to openly discuss the many contraception methods available with their patients. Sadly, unintended pregnancy with poor glycemic control is risky and greatly increases the chance of adverse pregnancy outcomes, including stillbirth, birth defects, preterm birth, and macrosomia (having a very large baby), so it’s really important that women living with diabetes plan for pregnancy.
That being said, deciding on a birth control method, can sometimes seem intimidating especially when you have what feels like a thousand other concerns. Believe me I know. In fact, I had such a bad experience with weight gain, insulin resistance, and depression that coincided with beginning a combination birth control pill in my teens, that it took me another five years before I decided to get an IUD (Mirena), which has worked wonderfully for the past three and a half years.
There’s not a ton of well-designed studies that have examined different forms of birth control, effects on blood glucose, and risk of complications, but I’ll try my best to break down some of the research that is available, as I go through some of the options.
Overview
The World Health Organization (WHO) categorizes the following contraceptive options in women with diabetes as follows:

The CDC released similar guidelines in 2016 including additional guidelines on LNG-IUD (hormonal IUD) and additional categorization for people who have had diabetes for more than 20 years.



Summary: The CDC and WHO guidelines are pretty much the same. Without complications most contraceptive methods are categorized as a 2 (the advantages generally outweigh the risks) with the exception of the category 1 copper IUD (No restriction).
IUD (Intrauterine Device)
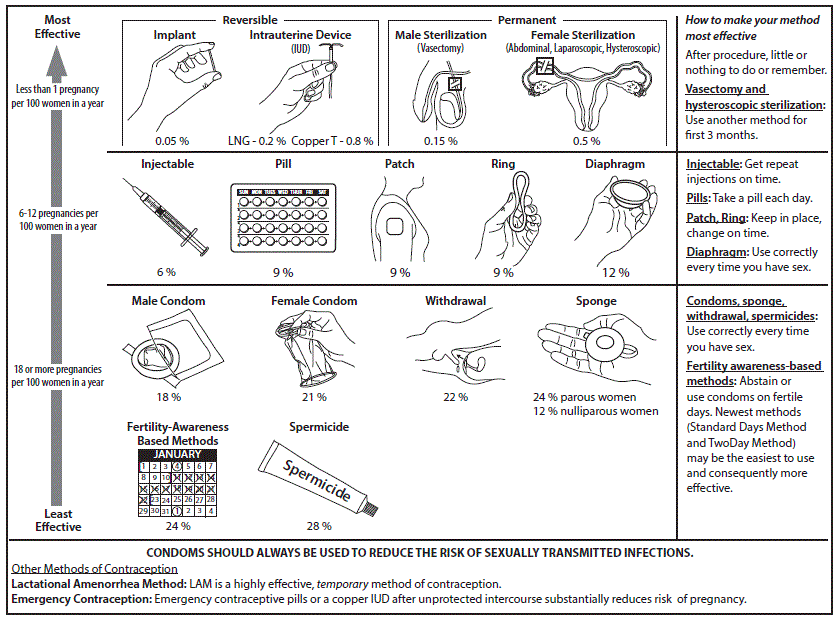
An IUD is a tiny T-shaped device inserted into the uterus to prevent pregnancy. It is considered one of the most effective forms of birth control available, and IUDs are considered both safe and effective for women with type 1 diabetes. There are two types of IUDs available:
- Copper IUDs (ParaGard)
- Hormonal IUDs (Mirena, Kyleena, Liletta, Skyla)- These release levonorgestrel, a progestin.
Copper (ParaGard) IUD versus Levonorgestrel-releasing (Hormonal) IUD
There’s not much difference when looking at blood glucose control. In a randomly controlled trial published in Obstetrics and Gynecology, participants with type 1 diabetes were randomly assigned to either levonogestrel-releasing (hormonal) IUD or copper IUD (ParaGard). Glucose control remained stable in both groups, and no significant difference in HbA1c was found between the groups (6.3%, +/- 1.5 compared with 6.3%, +/- 1.3). The same was true for mean fasting-serum glucose levels (7.4 mM, SD +/- 4.2 compared with 7.5 mM, SD +/- 4.2) and daily insulin doses (35.1 units, SD +/- 12.8 compared with 36.4 units, SD +/- 9.0). Also, no important differences were noted at either 6 weeks or 6 months. Interestingly enough, both groups experience very slight increases in serum blood glucose; however, HbA1c remained within the normal range, and daily insulin requirements did not increase over the 12 month study period.
The U.S. Medical Eligibility Criteria for Contraceptive Use ranks the copper IUD a category 1 (meaning no restrictions, method can be used) for insulin dependent diabetes compared with levenorgestrel-releasing IUD a category 2 (advantages generally outweigh theoretical or proven Risks). The copper IUD is the only category 1 contraceptive method for insulin dependent diabetics.
Combined Hormonal Contraception (CHC)
Combined hormonal contraception includes administration of both estrogen and progestogen/progestin. These include pills, patches, combined vaginal rings (such as the NuvaRing), and combined injectable contraception (DMPA, NET-EN). For years there were concerns about the effect of combined hormonal contraception on carbohydrate and lipid metabolism in women with diabetes; however, the research is inconclusive. Many reviews still suggest avoidance of CHCs in women with diabetes who have complications.
CHCs NOT Recommended with Complications
The research on CHCs in patients with type 1 diabetes is again inconclusive. This is an area of limited research, and there is not consistent evidence that use of combined hormonal contraception worsens glycemic control or microvascular complications. The guidelines suggest avoidance with cardiovascular risk factors such as cardiovascular disease, nephropathy, or active retinopathy. In a couple of studies conducted in a non-diabetic population, significantly higher glucose levels and insulin responses were observed with combination oral contraceptives.
CHCs are also not suggested for women with risk factors such as smoking, obesity, or hypertension due to the associated increased risk of venous thromboembolism, myocardial infarction and stroke. According to the CDC Criteria, CHCs are categorized as 3/4 (risks usually outweigh benefits/unacceptable health risk) in people with nephropathy (diabetic kidney disease), neuropathy, retinopathy, or who have had diabetes for more than 20 years.
Progestogen-only Pill (POP)
The Progestogen-only pill contains the hormone progestogen, and prevents pregnancy by thickening the mucus in the cervix to stop sperm from reaching an egg. It is important that this pill be taken daily within a set time period. This option is considered safe for women with diabetes with or without complications, and the WHO rates it a category 2 (the benefits generally outweigh the risks).
So, do Hormonal Contraceptives significantly impact glucose and lipid metabolism?
We don’t really know.
A Cochrane Systematic review published in 2013 looked at randomized controlled trials in women with diabetes. Four randomized controlled trials were included in the analysis. Although the authors did not find enough evidence to prove that hormonal contraceptives do or don’t impact glucose and lipid metabolism, the review did suggest that high-dose (30 µg ethinylestradiol + 75 µg gestodene, a progestogen) combined oral contraceptives (CHC) may slightly impair glucose homeostasis. There was also conflicting evidence when looking at lipid metabolism; however, copper IUD and progestogen-only oral contraceptives seemed to show slightly improved lipid metabolism. Again, this is an area that desperately needs more research… Hint hint to all my doctor and future Dr. friends.
In Sum:
Know your options, have an open discussion with your doctor, and don’t be afraid to ask questions!
Have an open discussion with your doctor.
For More Information See:
